
Osteoarchaeologists are experts in the study of human bone remains. Their techniques are employed by both archaeological and forensic specialists. This page will introduce you to the basics of Investigating Human Remains by way of skeletal remains.
Determining the Age of Human Skeletal Remains
Although children are generally smaller than adults, size on its own is not a reliable method of determining age. Skeletal size is only reliable before approximately 12 years of age. There are some key indicators that are of far more importance. For instance, the joints of the long bones have what are commonly referred to as "growth plates." These plates begin to fuse in girls (from 12 to 17 years of age) and in boys (from 15 to 21 years of age). As a general guide the stages of fusion can be used to determine the approximate age of adolescents. Epiphyses are those areas where bones fuse together. All long bones are composed of a diaphysis or shaft and two epiphyses or ends. The area between the diaphysis and the epiphyses is a layer or disk of cartilage known as an epiphyseal plate or disk. The various epiphyses fuse to the diaphysis at different ages. Many of the flat and irregular bones have epiphyses that fuse at standard rates. Having a list of standard fusion rates is very important in estimating the age of an unknown individual.
Prior to adolescence, one of the most commonly used age determinatives is found in dental development. As a broad rule of thumb, the first permanent molar erupts at age six, the second at twelve, and the third between the ages of 18-21. (More detail about the use of dental remains is given below).
Bones also show the wear of age. Osteoarchaeologists consider the thinning of bones, the more brittle internal structure, and the presence of certain age-indicating degenerative diseases such as osteoarthritis. (More detail is about the markers left on skeletal remains is given in a later paragraph).
Determining the Sex of Human Skeletal Remains
Unless puberty has been breached and some of the characteristics indicative of gender are present, it is often nearly impossible to determine the sex of preadolescents. By the same token, adults are more easy to deal with. However, it must be remembered that even adult human skeletal remains are highly variable. There is not always an easy distinction to be made between a small, somewhat effeminate man and a large, somewhat masculine woman. In short, abnormal hormonal levels can confuse the distinction.
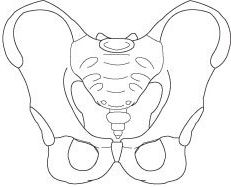
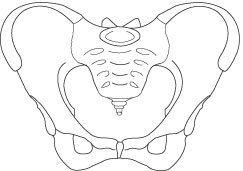
The best skeletal markers of sex are found in pelvic remains due to one of the major biological differences between men and women. The ability to carry and deliver babies and the skeletal variability caused by the hormonal changes during pregnancy, determines the shape of that part of the body. An adult woman's pelvis is wide and bowl-shaped; a man's is tall, narrow and more angular in appearance. The pelvis is made up of three bones (two innominates and the sacrum), this can be seen in the width of the sacrum, the sciatic notch and the sub-pubic angle, and sex can usually be determined even if part of the pelvis is destroyed.
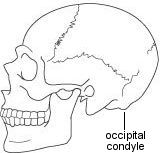
The skull is the next best indicator of sex. There are subtle differences in the shape of the eye sockets (orbits), the angle of the forehead is more vertical in women, the brow ridges and mastoid processes are smaller, and the muscle markings are less robust. In fact this is the main criterion for determining sex if only the long bones and a few fragments of skull remain - as a general rule men tend to be more physically robust than women.
The last indicator of sex is perhaps the easiest to imagine. This rule is often an oversimplification, so it isn't ever used as the sole marker for determining the sex of skeletal remains. When you look at the long bones of muscular people, the attachment points of these muscles are seen to have created a rough-hewn prominence on the shaft of these bones. The more robust the person was the more pronounced these ridges will appear. The smooth muscle tissue dominant in the majority of the female population precludes the development of these ridges.
Simplified General Rules of Thumb for Determining the Gender of Human Skeletal Remains
It is important not to depend on any single skeletal feature when attempting to establish gender from skeletal remains. You should always observe as many of the features of the remains as possible to increase the probability of success.
Cranial Differences
General Form & Shape:
In males, the overall construction of the skull is
heavier and more rugged looking than that of the female skull.
Eye Sockets: The orbits in the skull for the eyes are a bit squared in males,
while in females they are more rounded.
Brow Ridges: The supraorbital ridge of males is heavier and more pronounced
than it is in females; in females the brow is smooth and flat.
Cheekbones: The cheekbones of males are heavier and
more laterally arched; in females, the cheekbones are lighter, more compressed, and they
tend to lack the lateral arching.
Occipital Condyle: In males, the occipital bump at the rear base of the skull tends
to be much more pronounced than it is in females, where it can be almost nonexistent.
Chin Shape: The shape of a male's chin approximates the letter U, a
female's the letter V.
Jaw Line: The angle where the horizontal portion of the jaw curves upward
into the ramus, or vertical part of the jaw, is much more angular in males than it is in
females.



Differences in the Pelvis
General Form & Shape: The width of the pelvic girdle is broader in females than it is in
males. In females, the pelvic girdle surrounds a birth canal large enough for the fetus to
pass. In males, the pelvic opening is less round and open.
Pelvic Opening: The opening of the pelvis, called the pelvic inlet, is rounder
and larger in females, while in males it tends to be narrow and more constricted.
Pubic Arch: The joining of the bones at the bottom of the pelvis forms a
broad angle in females, usually greater than 90�, while in males it is narrow, usually
less than 90�.
Pubic Bone: In males, the pubic bone is roughly triangular in shape; in
females, it is rectangular.
For more information on this topic click here.
Measuring Parts of Human Skeletal Remains to Approximate the Whole
The type of measurements utilized to determine the "bigger picture" typically consists of the length, breadth and height of the skull and facial bones, and the lengths of long bones. Measurements are used to calculate the standard relationships between different dimensions. For instance, a cranial "slide rule" based on standard relationships found in the human skull can be used to calculated the relationship of the cranial vault. The forehead can then be divided into groups: narrow-, medium- and broad-headed.
The tools used include sliding and spreading calipers, osteometric boards to measure long bone lengths, and formula charts. Click here to view some examples.
The main purpose of measurement is comparison. Stature may be compared between groups or sexes. Often this shows some overlap between men and women, but not enough to negate the validity of certain generalizations among particular populations. Way back in the 1950s Trotter and Gleser created a chart of formulas for estimating the living stature of unknown individuals based the surviving long bones. Included below are some examples.
Estimation of Height Using the Femor:
Caucasoid Males (CM) 2.32 x length of femur in cm. + 65.53 = ______________(� 3.94 cm)
Caucasoid Females (CF) 2.47 x length of femur in cm. + 54.10 = ______________ (� 3.72 cm)
Marks of Trauma to Human Skeletal Remains
As grotesque as it might seem to contemplate such things, osteoarchaeologists and forensic pathologists have to think about whether visible trauma to the bones occurred at or near the time of death. Obviously, such an insight is important in determining the probable cause of death in unsolved criminal cases as well as the mysterious conditions archaeologists often find in ancient burial chambers. How is it possible to reconstruct anything based on skeletal trauma?
If living tissue continues tosurround the bone after the time of injury, osteoarchaeologists and forensic pathologists commonly refer to "green bone" trauma. The term "green" refers to the bone's relative flexibility and its healing capacity while still surrounded by living tissue. "Dry bone", on the other hand, will splinter or crush in a distinctly different way. Wounds inflicted upon a corps do not have the same appearance, even if the bone is surrounded by flesh at the time of the trauma. If Mr. X were to receive a crushing blow to the collar bone which sent him over the edge of a precipice to his death on the rocks along the shallows of a river 300 feet below, it is possible to differentiate these initial injuries from those sustained 3 days later when the spring rains came, swelled the river, and carried the body over a series of severe rapids--breaking numerous bones along the way to Mr. X's final resting spot where some hapless traveler came upon his body. Due to the same "green bone" characteristics, we also know from many interesting mesoamerican skeletal remains that living humans had survived (apparently for many years) some sort of primitive "cranial surgery." In other instances archaeologists have found remains of Roman soldiers with multiple cranial fractures that show some soldiers of a particular garrison survived long after they sustained these injuries, whereas other soldiers died by similar blows to the skull. In the latter case, the skull was "green." The skull demonstrates a "bending" in its structure that would not be possible in the case that it was not surrounded by living tissue at the time the trauma was inflicted. Knife or bullet wounds to the bone that are inflicted close to the time of death also exhibit "green" characteristics.
Other Traits Sometimes Considered
Metopism -- the frontal bone of the skull is divided into two halves in the newborn infant, and eventually fuses together between the ages of 2 and 6 years. Sometimes fusion does not take place, and a meanering suture remains in place of the original division. This trait is nearly exclusive to caucasoid populations.
Wormian bones --these are extra bones which occur between the plates of the skull vault. This trait is most common among American Indian populations.
Tiny Hornlike Bones and Ridges --a torus may occur in the center line of the palate, on either side of the maxilla, on either side of the mandible, or in the ears. These anomalies are bony protuberances which appear to be genetic in origin. Mandibular tori are known to be particularly common in some groups of people, particularly the Inuit. Auditory tori have recently been associated with swimming by some leading osteoarchaeologists.
Parietal Holes--Other cranial traits include the presence or absence of certain holes, particularly those on the parietal, and around the eye sockets. Some of these traits are so common that it is more unusual not to find them.
Elbow Joint Hole --a small hole sometimes forms at the elbow joint in the distal end of the humerus. This tends to occur more often in female skeletons and may be related to robusticity.
Femoral Third Trochanter-- "trochanter" is the term for one of three processes which form on the femur. The greater and lesser trochanters are present in normal anatomy, but a third trochanter is unusual. It forms at the back of the bone just below the hip joint, near the attachment for the gluteal muscle. In some groups it is more common in men, and may be related to robusticity.
Vertebral Traits --there are many possibilities for variety within the human spine. Sometimes there are more or less vertebrae than normal, for example 13 thoracic vertebrae instead of the usual twelve. Sometimes ribs may form on the last cervical or first lumbar vertebrae, or the vertebral arch may not fuse to the body.
Utilizing Dental Markers
Dental analysis involves recording the state of eruption, tooth loss (before or after death) and dental pathology for each tooth in the mouth. This data can then be used to calculate the prevalence of dental disease within a group of skeletons. It can sometimes lead to conclusions about a common diet or dietary patterns.
The most common findings include dental caries, abscesses and teeth lost during life. Not yet erupted or impacted wisdom teeth are also common. Tatar is common among many individuals, and some have a condition known as enamel hypoplasia (lines or pits in the enamel related to malnutrition or illness as a child). Other anomalies include the retention of a "milk tooth" among fully developed adult teeth, overcrowding, or abnormally small teeth.
Study of the teeth is useful in showing changes in dental health. Different rates of dental disease can be seen in different age groups, with the oldest members of a population generally being most affected by dental disease and tooth loss. Dietary information may be obtained from the teeth.
Of course, the use of dental charts and x-rays are extremely useful in idenfying remains. Perhaps the most infamous case is that of Adolf and Eva Hitler.
One of the more recent ways developed for determining the approximate age of adults is the degree of transparency in the lower root portion of the dentin. As we age more and more of the lower extremity of the dentin turns transparent. Using large samples of molars of different age groups between 21 and 90 osteoarchaeologists and forensic pathologists have created a sliding scale for determining approximate age.
Disease Sometimes Leaves its Mark
The study of ancient diseases is called Palaeopathology. Palaeopathology has some important intersections with osteoarchaeology. A number of secondary sources including documents, art, and medical instruments can be useful in interpreting marks left behind on ancient bones. Some palaeopathologists are able to use soft tissue evidence from mummified remains. Unfortunately, for osteoarchaeologists, most disease does not reach the bone. Evidence for illnesses such as measles, smallpox, plague, influenza, and many others just isn't manifested in human bone remains. The one obvious exception is that of bone diseases, fractures and wear.
The following categories are typical examples that can make their mark on the skeletal system:
Congenital Diseases
These include mild conditions such as spina bifida occulta of the sacrum, cervical ribs,
extra vertebrae, etc.
Arthropathies and Degenerative Disease
These are the most common diseases to be found in skeletal material, and include
osteoarthritis, osteoporosis, and general changes associated with the aging process.
Spinal Conditions
The spine is a common area for stress injuries and pain, mainly due to our bipedalism.
Metabolic and Nutritional Disorders
Bone is easily affected by poor nutrition, and produces changes related to iron deficiency
anemia and Vitamin D deficiencies such as rickets. Other changes which may be related to
malnutrition or illness can be seen in the teeth (enamel deficiencies and abnormalities)
and the long bones (Harris lines).
Circulatory Problems
If the blood supply to an area of bone is cut off, that area of the skeleton will become
necrotic (dead).
Infectious Diseases
Not many infections reach the bone. Acute diseases such as the plague and smallpox tend to
kill or cure very quickly and do not have time to affect the skeleton. Chronic illnesses
such as tuberculosis, leprosy and syphilis can be recognized in human remains.
Trying to Determine Race from Skeletal Remains
The notion that race is "only skin deep" is not necessarily the case. The race of skeletal remains can often be determined by osteoarchaeologists and forensic pathologists with a high degree of certainty. Figuring the race of skeletal remains is not only important to longstanding historic debates about ancient cultures, but is equally significant to the crime scene investigators working to discover the identity of many an unnamed homicide victim. The problem is that there is much variation even within seemingly homogenous racial groups; therefore, osteoarchaeologists must look for several markers that are pronounced in one racial group. Difficulties also arise due to the blending of races through intermarriage Osteoarchaeologists are not out to prove the superiority or inferiority of racial characteristics, their task is instead to reconstruct a more accurate anthropology. For example, the skeletal characteristics of Mongoloids (Eskimo, American Indians, and Asians) often include very forward projecting cheekbones and comparatively flat faces, eye sockets that are more circular than those of other groups, a nasal aperture that is moderate in width, shovel-shaped incisors, and usually quite curved femora (upper leg bones) with considerable twisting of the neck of the bone. The skulls of Africans tend to have little or no projection of the cheekbones, rectangular eye sockets that are wide apart compared to other groups, broad nasal aperture, prognathism, or jutting forward of the lower face, and relatively straight femora with very little twisting of the head or neck of the bone. Some features of Caucasoid skeletons include markedly recessive cheekbones, faces that are sharper or more pointed than those of other groups, a narrow nasal aperture, and femora that are intermediate between those of Mongoloids and Africans in both curvature and twist.
Some excellent information about racial differences in the skeletal system can be found by clicking here.

